Official Massachusetts Claim Template
Key takeaways
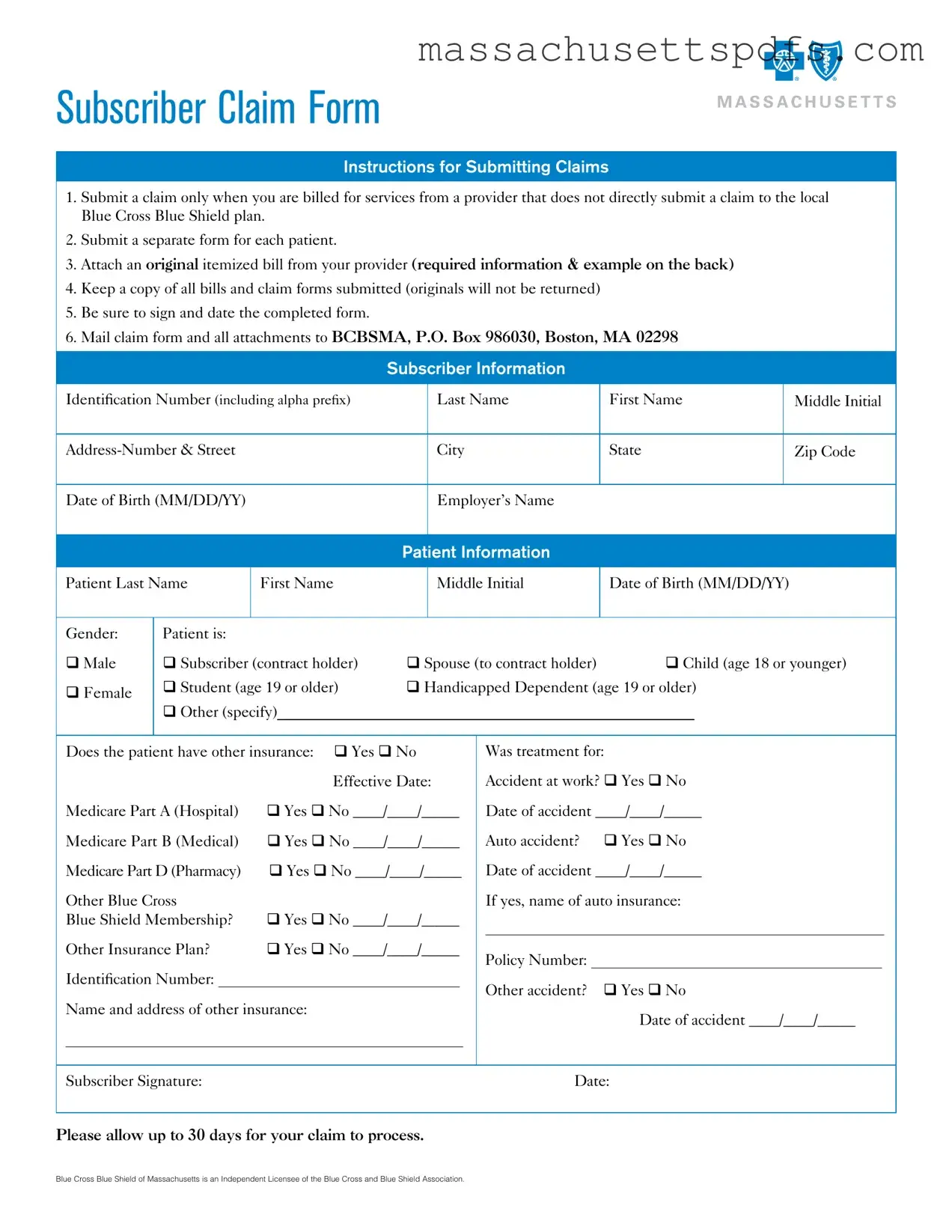
When filling out and using the Massachusetts Claim form, consider the following key takeaways:
- Submit claims only when necessary: Use the claim form only if the provider does not directly submit a claim to the local Blue Cross Blue Shield plan.
- One form per patient: Each patient requires a separate claim form to ensure proper processing.
- Include an itemized bill: Attach an original itemized bill from the provider, which must contain specific required information.
- Keep copies: Retain copies of all submitted bills and claim forms, as originals will not be returned.
- Sign and date: Ensure the completed form is signed and dated before mailing it to the specified address.
Following these guidelines will help streamline the claims process and ensure that all necessary information is provided for a successful submission.
Documents used along the form
When submitting a claim using the Massachusetts Claim form, several other documents may be required to support your claim. Each of these documents serves a specific purpose and helps ensure that your claim is processed efficiently.
- Itemized Bill: This document must be an original bill from the healthcare provider. It should include detailed information about the services provided, such as the provider’s name, address, and Tax ID, along with the date of service, procedure codes, and charges.
- Explanation of Benefits (EOB): If you have other insurance, the EOB from that insurer outlines what services were covered and how much was paid. This document is crucial for determining any remaining balance that your current claim may cover.
- Divorce Settlement Agreement: To efficiently navigate the divorce process, refer to the essential Colorado Divorce Settlement Agreement guidelines for outlining asset division and other critical obligations.
- Medicare Summary Notice (MSN): For patients eligible for Medicare, the MSN provides details about services received and the amounts covered by Medicare. This notice can help clarify what portion of the costs you are responsible for.
- Prescription Drug Receipt: If your claim includes prescription drugs, an itemized receipt from the pharmacy is necessary. This receipt should list the National Drug Code, the name of the drug, the date dispensed, and the quantity.
- Accident Report: If the treatment was related to an accident, a report detailing the circumstances of the accident may be required. This document helps establish the context of the claim and any liability issues.
Ensuring you have these documents ready will facilitate a smoother claims process. Always keep copies of everything submitted for your records.
Document Information
| Fact Name | Details |
|---|---|
| Submission Requirement | Submit the claim only when billed for services from a provider that does not directly submit a claim to the local Blue Cross Blue Shield plan. |
| Separate Forms | Each patient requires a separate claim form for submission. |
| Itemized Bill | An original itemized bill from the provider must be attached. It should include required information as outlined in the instructions. |
| Document Retention | Keep copies of all bills and claim forms submitted, as originals will not be returned. |
| Signature Requirement | Ensure that the completed form is signed and dated by the subscriber. |
| Mailing Address | Send the claim form and all attachments to BCBSMA, P.O. Box 986030, Boston, MA 02298. |
Popular PDF Forms
Ma 355s - Excise tax calculations commence with the total due from financial institution members.
For those looking to navigate the process of boat ownership transfer, using the New York Boat Bill of Sale form is essential, and you can find helpful resources like PDF Templates to ensure everything is filled out correctly.
Form M-941 - Employers from various industries must adhere to filing the M-941 if they withhold taxes.
Withholding Tax Form M-941 - The M-941A helps in keeping withholding tax accounts organized and updated.
Guide to Writing Massachusetts Claim
Filling out the Massachusetts Claim Form requires careful attention to detail. Once you have completed the form, you will need to submit it along with any required attachments to ensure your claim is processed efficiently. Below are the steps to guide you through the process of filling out the form correctly.
- Begin by obtaining the Massachusetts Claim Form.
- Fill in your Subscriber Information:
- Identification Number (including alpha prefix)
- Last Name
- First Name
- Middle Initial
- Address (Number & Street)
- City
- State
- Zip Code
- Date of Birth (MM/DD/YY)
- Employer’s Name
- Next, complete the Patient Information section:
- Patient Last Name
- Patient First Name
- Patient Middle Initial
- Patient Date of Birth (MM/DD/YY)
- Select Gender: Male or Female
- Specify Patient Status (Subscriber, Student, Spouse, Child, or Handicapped Dependent)
- Indicate if the patient has other insurance (Yes or No)
- If yes, provide the Effective Date and details for Medicare Part A, Part B, Part D, and any other insurance plans.
- Indicate if treatment was for an accident:
- Specify if it was an accident at work, auto accident, or other accident and provide the respective dates.
- If applicable, include the name of the auto insurance and policy number.
- Attach an original itemized bill from your provider. Ensure it includes all required information such as provider details, patient name, dates of service, itemized charges, procedure codes, diagnosis codes, and units.
- Review the completed form for accuracy. Make sure to sign and date the form.
- Keep a copy of all documents for your records, as originals will not be returned.
- Mail the completed claim form and all attachments to: BCBSMA, P.O. Box 986030, Boston, MA 02298.
After submitting your claim, please allow up to 30 days for processing. You can check the status of your claim online by visiting the Blue Cross Blue Shield of Massachusetts website.
Similar forms
-
Insurance Claim Form: Similar to the Massachusetts Claim form, an insurance claim form is used to request payment for medical services from an insurance provider. Both require detailed information about the patient and services rendered.
-
Medicare Claim Form (CMS-1500): This form is utilized by healthcare providers to bill Medicare for services provided. Like the Massachusetts Claim form, it requires patient information, service details, and provider identification.
-
Health Insurance Portability and Accountability Act (HIPAA) Release Form: This document allows healthcare providers to share patient information with insurance companies. Both forms ensure the proper handling of patient data and consent.
- California Vehicle Purchase Agreement: This form is essential for any vehicle sale in California, as it outlines the terms and conditions agreed upon by both parties. It includes critical details like the vehicle's price and condition, ensuring clarity and protection for both the buyer and seller. For more information, you can visit My PDF Forms.
-
Workers' Compensation Claim Form: Used to claim benefits for work-related injuries, this form is similar in that it requires detailed information about the incident and services provided, just like the Massachusetts Claim form.
-
Auto Insurance Claim Form: This form is filled out to seek compensation for medical expenses resulting from auto accidents. Similar to the Massachusetts Claim form, it requires details about the accident and treatment.
-
Prescription Drug Claim Form: This document is used to request reimbursement for prescription medications. It shares similarities with the Massachusetts Claim form, particularly in requiring itemized receipts and service details.
-
Flexible Spending Account (FSA) Claim Form: Used to reimburse eligible medical expenses, this form is akin to the Massachusetts Claim form in that it requires itemized bills and patient information.
-
Health Savings Account (HSA) Claim Form: Similar to the FSA form, it allows individuals to claim medical expenses for reimbursement. Both require proof of expenses and patient details.
-
Third-Party Liability Claim Form: This form is used when another party is responsible for medical costs. Like the Massachusetts Claim form, it requires comprehensive details about the incident and treatment received.
-
Patient Authorization Form: This document grants permission for healthcare providers to share medical information with insurers. It is similar to the Massachusetts Claim form in ensuring that patient consent is obtained for claims processing.